

Bone Grafting
Bone loss can occur in the upper and lower jaws for several reasons. Localized bone loss often occurs around diseased teeth due to periodontal (gum) disease, fractured teeth, traumatic injuries and dental infections. In addition, over a period of time the jawbone associated with missing teeth atrophies (bone resorption/shrinks). This often leaves a condition in which there is poor quality and quantity of bone, unsuitable for placement of dental implants. In the past, patients with significant bone loss were not candidates for placement of dental implants.
With current bone graft techniques, we have the ability to grow bone where needed. Augmentation bone grafts can be accomplished virtually anywhere on the upper and lower jaws. This enables us to offer dental implants as a replacement for missing teeth to almost all patients, even if substantial bone loss has occurred.
Commonly used bone graft materials include autogenous bone (your own bone), cadaver bone (bank bone), bovine bone and synthetic bone. The selection of graft material and surgical technique are based on the location and severity of the bone loss. In most cases, specially prepared cadaver bone and/or autogenous bone are utilized. Autogenous bone is usually taken from other areas of the upper or lower jaw.
The great majority of bone grafts required for implant placement are minor procedures which can easily be accomplished in the office under local anesthesia or intravenous sedation. Major bone grafts are utilized to repair extremely large defects of the jaws. These major defects usually result from severe traumatic injuries, tumor surgery, and congenital defects. Large defects are always repaired using the patient’s own bone. Since a large amount of bone is needed to repair these extensive defects, the bone must be harvested from areas where there is an abundance of available bone. This bone can be harvested from a number of different sites depending on the size of the defect. The skull (cranium), hip (iliac crest), and lateral knee (tibia), are common donor sites. These procedures are performed in an operating room and require a hospital stay.
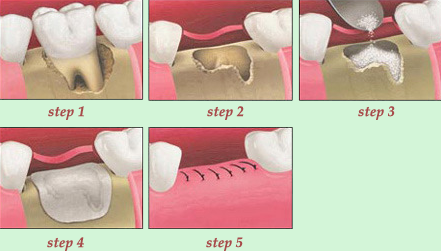
Socket Preservation Graft
The socket preservation graft is an extremely simple and important bone graft procedure. This procedure must be accomplished at the time of tooth extraction. It helps to preserve bone at an extraction site in preparation for future implant placement. The area of the jaw bone that holds a tooth in place is called a tooth socket. Preservation of bone volume and architecture (shape) is crucial for implant stability and esthetics. After a tooth has been extracted, the supporting bone (socket) begins to rapidly melt away (bone resorption). Post-extraction bone resorption tends to be particularly severe in sockets with thin walls of bone. A socket preservation graft placed immediately after tooth extraction helps to preserve bone volume and architecture by minimizing post-extraction bone resorption. This procedure diminishes the likelihood that a more complicated bone graft will be necessary prior to implant placement. In many cases, this simple graft is all that is required to provide sufficient bone for implant placement. In some cases, due to severe inflammation at the extraction site, a low maxillary sinus, extensive preexisting bone loss and/or diseased tissue at the extraction site, it is not possible to provide enough bone volume for implant placement with this procedure alone. In these circumstances additional bone grafting may be required either at the time of implant placement, or as a staged procedure prior to implant placement.
The tooth is extracted with great care leaving as much socket bone intact as possible. After the tooth has been extracted, the socket is gently but thoroughly cleaned and debrided. A specially prepared particulate cadaver bone graft is inserted into the socket and retained in place with a with a small collagen plug which is sutured over the socket. The collagen plug falls out by itself a week or two later, the sutures dissolve and fall out in two to three weeks. The site is reevaluated for implant placement four months after grafting; if sufficient bone is present the patient is ready to be scheduled for implant surgery.